
Linking the Environment and Human Health
Alexander is working to develop a tree-based health intervention with local nonprofit Trees Durham.
Growing recognition of the relationship between global climate change and human health has led to a greater emphasis on the responsibility of clinicians and health systems to incorporate a climate lens into their practice. The intimate link between the environment and human health has many dynamic mechanisms affecting both health outcomes and health disparities. This lens adds emphasis to the vital work of Trees Durham, a local nonprofit organization. Trees Durham is an environmental justice group that is dedicated to combating climate change and creating environmental equality across Durham. The goals of the organization are to take direct action to (1) plant & preserve trees, (2) combat climate change, and (3) create environmental equity.
Recent research has supported the positive effects of urban green space and tree canopy coverage on patient-level health outcomes such as cardiovascular and respiratory disease, immune function, and mental health. In addition, epidemiological analyses have demonstrated that populations are at lower risk of mortality when they reside in areas with more green space. Beyond direct health implications, tree canopy coverage has an added benefit of increasing residents’ sense of community connectedness and reducing crime rates. Finally, trees are among the most effective tools for taking care of our global community, capturing carbon from the atmosphere, and limiting the rise of CO2 emissions.
In urban areas across the United States, tree canopy coverage is not equally distributed and often aligns with well-known health disparities. In Durham County, where tree canopy coverage is 52% (Figure 1A), lowest coverage is found in districts historically red-lined in the 1930s (Figures 1B and 2), according to an analysis done by Duke’s Nicholas School of the Environment. Policies like redlining perpetuate a pattern of inequity across social, economic, and health strata, ultimately manifesting as structural racism. Durham residents in these districts are disproportionately non-white, have lower median household income, are more likely to be renters, and suffer from worse health outcomes. Cardiovascular is of particular interest as the incidence of heart attack is four times higher in areas affected by these historical discriminatory policies. This is important in light of the 2017 Durham Community Needs Assessment, which identified cardiovascular disease as the second leading cause of death in the county, affecting more than 35% of residents and making it one of the “most widespread and costly health problems facing Durham County.”
The goal of our project is to develop an evidence-driven and community-based intervention to purposefully plant trees in Durham communities that would benefit the most. An additional ambitious goal of our work is to directly combat historical racist policies that dictate the health and wellbeing of our city’s most marginalized communities and to provide an example for how to implement city planning interventions with a health equity framework.
Finally, this work has tremendous meaning for my vocation as a medical student and as a future physician. The essential reflection is that the health of the patients I work with now and my future patients is shaped by many factors outside the clinic, such as the environment in which they live. Moreover, their health outcomes are affected by historical context, including discriminatory policies from nearly 100 years ago. Together, these reflections expand what needs to be considered in the clinical interaction beyond counseling on what diagnostic tests or prescription medicines are needed to include more robust context of the patient.
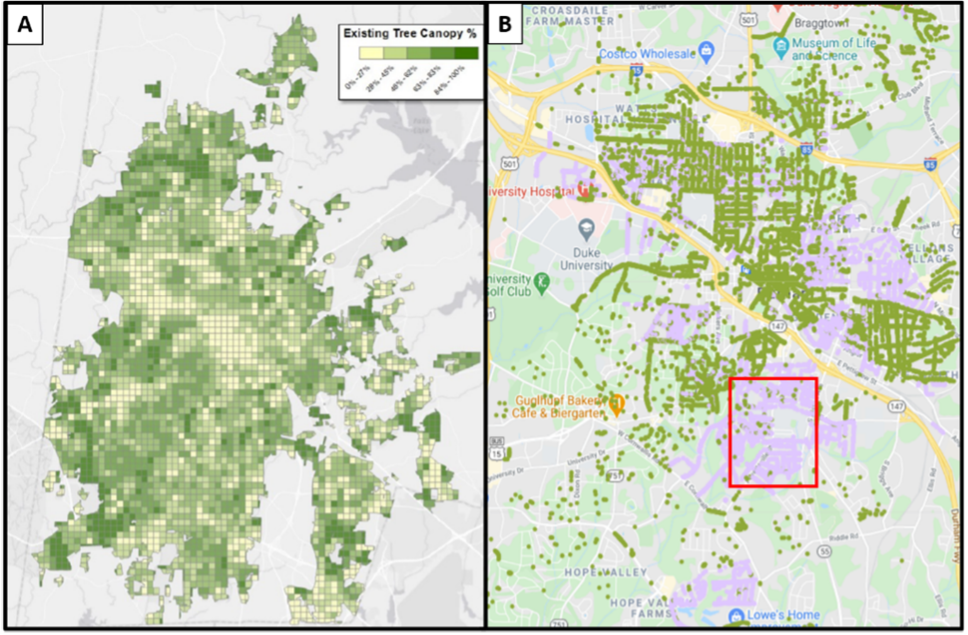 Figure 1.
Figure 1.
A – Durham County tree canopy coverage map, summarized by 1000-foot grid cells. Derived from LiDAR by City of Durham.
B – Street tree sites in Durham. The green dots represent sites with trees and the purple dots represent sites that are available. The red designates preliminary target sites. (Adapted from City of Durham and Trees Durham)

Figure 2.
Comparison of tree canopy coverage in 2015 among Durham risk class zones delineated by the Homeowners Loan Corporation in the 1930’s. (Adapted from Swenson et al. 2020)